Airborne Virus Concerns

The Problem: Transmission of SARS-CoV-2 is predominantly through inhalation
A recently published research paper from the Department of Environmental Health Sciences of University of Michigan School of Public Health examined the potential infection risks of people exposed to SARS-CoV-2 virus in publicly accessible non-healthcare environments, concluding that inhalation is the predominant route of exposure compared to surface contact.
These authors also estimated the risk of airborne transmission to be 20,000 times higher than from contact with contaminated surfaces. This further underscores the U.S. Centers for Disease Control and Prevention’s (CDC) statement that the principal mode by which people are infected with SARS-CoV-2 is through exposure to respiratory droplets carrying the infectious virus.
This article is the first in a series from Grignard. Access part two here and read part three here.
The Solution: Reduce the immediate level of inhaled viral load
On January 15, 2021, the U.S. Environmental Protection Agency (EPA) issued a Section 18 Emergency Exemption for the use of Grignard Pure® as the first-of-its-kind airborne antiviral effective at killing more than 98.5% of the SARS-CoV-2 virus in the air. Grignard Pure is a proprietary mixture containing the active ingredient triethylene glycol (TEG). It is aerosolized and dispersed into the air via a handheld or portable device. The EPA issued a one-year renewal of the Emergency Exemption on January 15, 2022.
In a recent study, currently under peer review, researchers, including independent members of Grignard Pure LLC’s science advisory team, reported on the effectiveness of Grignard Pure to inactivate the bacteriophage MS2 (the virus—a non-enveloped viral microbe used widely as a SARS-CoV-2 surrogate). The authors reviewed the results of extensive efficacy testing undertaken by two accredited third-party labs, which the company had submitted to the EPA.
The objective of the efficacy testing was to measure the reduction in airborne concentrations of viable virus in the presence of differing Grignard Pure aerosol concentrations ranging from 0.02 mg/m3 to 0.5 mg/m3. Measurements were taken at 30 seconds and 15, 60, and 90 minutes. To account for natural die-off and settling of the virus over time, these measurements were compared with measurements at the same time points of the levels of the virus in the air without any Grignard Pure.
Two protocols were employed:
- Episodic treatment: Introducing aerosolized Grignard Pure into the air containing the virus, using a single shot, 4-second spray (using a vaporizer or nebulizer)—to simulate “episodic” treatment of indoor spaces such as hotel rooms, break rooms, classrooms, movie theatre auditoriums, or rental cars.
- Continuous treatment: Introducing virus into air containing Grignard Pure, in a controlled time release where Grignard Pure was dispersed to maintain a consistent concentration, to simulate “intermittent” treatment of indoor spaces, where a device could be placed to provide “continuous” dispersion (delivered intermittently to maintain the proper level of concentration in the air).
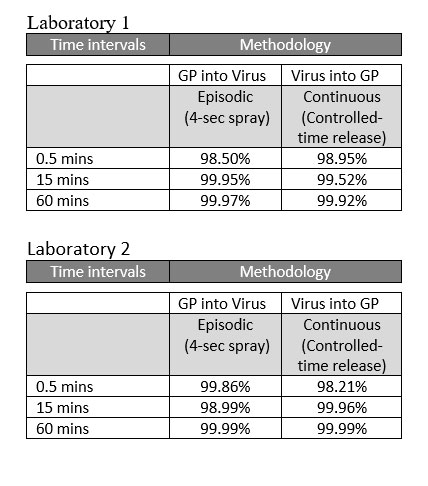
Results
The tests clearly demonstrated the efficacy of Grignard Pure at aerosol concentrations between 0.02 mg/m3 and 0.5 mg/m3 (corresponding to TEG aerosol concentrations of 0.01 mg/m3 to 0.29 mg/m3) to significantly reduce virus concentrations (i.e., airborne viruses). EPA’s approval allows Grignard Pure (GP) to be used in occupied indoor spaces to provide an added layer of protection by reducing the levels of airborne virus.
The tables below show the percentage reduction of the virus in the air at three-time intervals (0.5 min, 15 min, 60 min) from experiments done in two different laboratories.
Looking ahead
Grignard Pure is currently working to secure permanent approvals from the EPA for use against multiple airborne pathogens and mold spores in both unoccupied and occupied indoor spaces.
You can read the complete science paper here.
Links to independent health and safety assessments:









{kind=link}
{kind=link}